

{kind=link}
{kind=link}
-

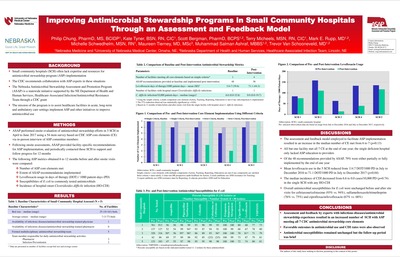
Improving Antimicrobial Stewardship Programs in Small Community Hospitals Through an Assessment and Feedback Model
Philip Chung, Kate Tyner, Scott Bergman, Terry Micheels, Mark Rupp, Michelle Schwedhelm, Maureen Tierney, Muhammad Salman Ashraf, and Trevor Van Schooneveld
Small community hospitals often lack expertise and resources for antimicrobial stewardship program implementation. Using an assessment-and-feedback model, Nebraska ASAP performed onsite assessment of antimicrobial stewardship efforts in 5 small community hospitals and provided facility specific feedback on implementation/augmentation of antimicrobial stewardship program. As a result of this model, participating small community hospitals were able to increase the number of antimicrobial stewardship core elements implemented while reducing antibiotic use and incidence of CDI.
-

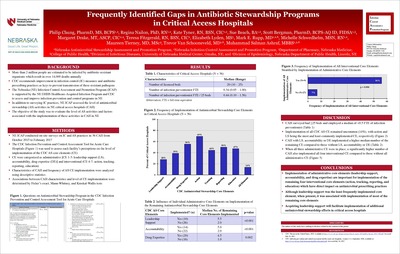
Frequently Identified Gaps in Antibiotic Stewardship Programs in Critical Access Hospitals
Philip Chung, Regina Nailon, Kate Tyner, Sue Beach, Scott Bergman, Margaret Drake, Teresa Fitzgerald, Elizabeth Lyden, Mark Rupp, Michelle Schwedhelm, Maureen Tierney-Brenran, Trevor Van Schooneveld, and Muhammad Salman Ashraf
Background: Nebraska (NE) Infection Control Assessment and Promotion Program (ICAP) is a CDC funded project. ICAP team works in collaboration with NE Department of Health and Human Services (NEDHHS) to assess and improve infection prevention and control programs (IPCP) in various health care settings including resource limited settings like critical access hospitals (CAH). Little is known about the existing gaps in antimicrobial stewardship programs (ASP) of CAH. Hence, we decided to study the current level of ASP activities and factors associated with these activities in CAH.
Methods: NE ICAP conducted on-site surveys in 36 CAH from October 2015 to February 2017. ASP activities related to the 7 CDC recommended core elements (CE) including leadership support (LS), accountability, drug expertise (DE), action, tracking, reporting, and education were assessed using a CDC Infection Control Assessment Tool for acute care hospitals. Descriptive analyses evaluated CAH characteristics and frequency of CE implementation. Fisher’s exact, Mann–Whitney, and Kruskal–Wallis tests were used for statistical analyses examining the association of various factors with level of ASP activities.
Results: The 36 surveyed CAH had a median of 20 (range 10–25) beds and employed a median of 0.4 (range 0.1–1.6) infection preventionist (IP) full-time equivalent (FTE)/25-bed. Frequency of CE implementation varied among CAH with action and LS as the most (69%) and least (28%) frequently implemented elements, respectively. Close to half (47%) of surveyed CAH had implemented ≥4 CE but only 14% of facilities had all 7 CE. Median bed size and IP FTE/25-bed were similar among CAH with 0–2, 3-5, or ≥6 CE in place. CAH with LS or accountability for ASP implemented higher median numbers of the remaining CE compared with CAH without LS or accountability (5 vs. 2, P < 0.01 and 4 vs. 2, P < 0.01, respectively). Facilities with The presence of LS, accountability and drug expertise were more likely to have all 4 remaining CE implemented than others (56% vs. 8%, P < 0.01).
Conclusion: LS, accountability, and DE are important factors for the implementation of the remaining 4 CE in CAH. Although LS was the least frequently implemented CE, when present was associated with implementation of most of the other CE. Acquiring LS will facilitate implementation of additional ASP efforts in CAH.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.